Contribute
| Technology - Better Management For Women At Elevated Risk For Breast Cancer |
Kevin S. Hughes, MD
08/08/2006
This year approximately 1.2 million women worldwide will be diagnosed with breast cancer, and over 400,000 women will die from the disease. With earlier detection, significantly higher cure rates are possible. The challenge is to identify and appropriately manage women at elevated risk. We already have in place a number of the pieces of this public health puzzle. We know what factors place a woman at higher risk, and we can offer strategies to help decrease her risk and/or to try to catch her disease at an earlier, more treatable phase.
Who is at elevated risk? Women at high risk include those who have a family history of breast or ovarian cancer and women with certain biopsy diagnoses. Women are considered to have a high-risk family history of breast cancer if they have some or all of the following characteristics.
• Multiple relatives with breast or ovarian cancer
• Relative 40 years of age or younger at diagnosis
• Relative with bilateral breast cancer or breast and ovarian cancer
• Male relative with breast cancer
We tend to lower the threshold of suspicion somewhat for women of Ashkenazi Jewish descent, because they are more likely than women of other ethnicities to carry the BRCA1 and BRCA2 genetic mutations associated with increased risk for breast and ovarian cancer.
Also, women who have a pathologic diagnosis of atypical hyperplasia or lobular carcinoma in situ are at elevated risk for breast cancer. They should be closely monitored and may benefit from more aggressive management.
At a specialized center like the Avon Foundation Comprehensive Breast Evaluation Center at Massachusetts General Hospital, our specialists not only identify and stratify risk, but also customize management strategies appropriate to each woman’s level of risk.
These may include:
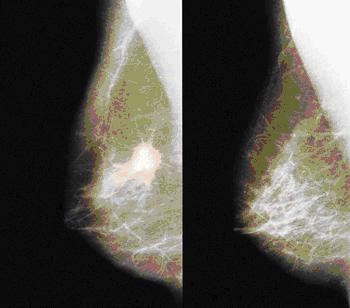
Breast imaging. We work closely with Daniel Kopans, MD, Director of Breast Imaging at the Avon Center, and his colleagues to offer the most appropriate breast imaging techniques for each woman. For women at significantly elevated risk, we recommend changing the usual mammographic screening pattern and beginning yearly screening as early as age 25 instead of age 40.
MRI is quite sensitive in detecting breast cancer, but it also detects non-cancerous abnormalities as well, leading to more biopsies. Experts are considering how best to fit this imaging technique into our armamentarium. Currently, we offer MRI screening selectively, and almost exclusively to known mutation carriers. This practice may change as we gather more knowledge in the area.
More frequent physical examinations. For high-risk women, we often recommend a breast exam by a physician every six months.
Tamoxifen. We recommend prophylactic tamoxifen to patients with atypical hyperplasia or lobular carcinoma in situ. We discuss tamoxifen with women who have a strong family history, but it is less clear that the drug has a protective effect in this population
Prophylactic mastectomy. This may be an option for women with a known mutation of BRCA1 or BRCA2 gene. Even in this population, it is performed only under very selected conditions.
Ovarian cancer. Women with a genetic susceptibility to breast cancer are also at increased risk for ovarian cancer, so we recommend a number of screening and preventive options to address their risk for ovarian cancer, as well. These include use of oral contraceptives, which are very effective in decreasing the risk of ovarian cancer; screening with transvaginal ultrasound and CA-125 blood levels, although these lack optimum specificity and sensitivity; and prophylactic oophorectomy for mutation carriers.
Genetic counseling. Genetic counseling can be a useful tool in risk assessment. My colleague Paula Ryan, MD, PhD, Medical Director of the Breast and Ovarian Cancer Genetics Program at the Massachusetts General Hospital Cancer Center, says genetic counseling should be considered in women with a family history of the disease. Genetic testing may be offered as part of the counseling process and is useful in further stratifying women at risk and identifying appropriate management strategies. Genetic counseling services are available through the Cancer Center’s Center for Cancer Risk Analysis.
Population-based identification and management. Clearly, we have the tools to identify women at elevated risk for breast cancer and can offer a number of screening and preventive options. The larger challenge will be applying those tools. As part of the care at the Avon Center, family history is taken when a woman has a mammogram. We are trying to determine how best to use this information to provide patients with more precise risk stratification and to advise patients as to the need for more intensive screening or more aggressive management.
To apply this process to the entire population of women in a clinically useful way will be a huge undertaking. We will need to find ways to identify women who do not have mammograms. We will need to find the best ways to get information regarding her personal risk stratification back to each patient. If the patient requires further management, we will need to identify the best ways to involve her PCP in her continuing management. And we will need to find ways to deal with the sheer volume of women who require more screening, more counseling, and more treatment.
We are poised to embark on a study with four or five primary care practices to begin to answer some of these questions. If we can describe a population-based process for identifying and managing women at high risk for breast cancer, it will undoubtedly save lives. In addition, it may be a useful model for wide-scale screening for other cancers, as well.
This article is provided by Partners HealhCare.
You may also access this article through our web-site http://www.lokvani.com/